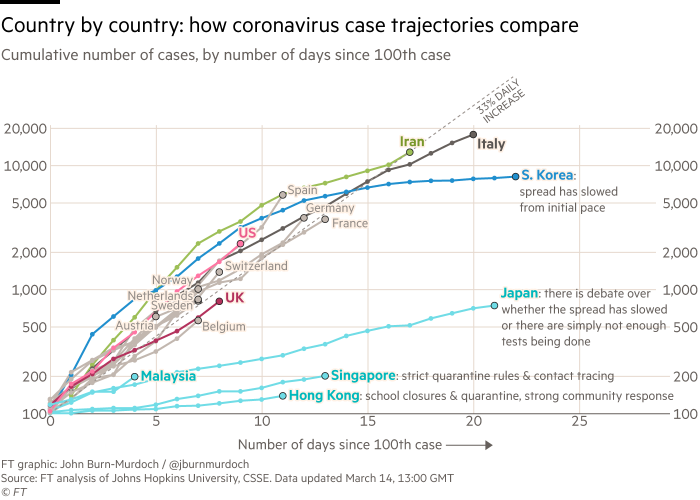
That is the most useful graph on this subject so far. Go look at it now.
Most countries have exactly the same growth trajectory measured from 100 cases. That's solid data about how this behaves.
Singapore and Hong Kong have been able to slow things down by strong measures, but it's still a straight line on a log graph, just with 1/3 of the growth rate. Italy is on the same line, just 8 days ahead of Europe and 13 days ahead of the US.
I still don't get how people - including apparently some governments - don't get or don't believe it. Getting this graph is as simple as 1) taking the daily measurements, and 2) plotting them on log scale (and technically 3) shifting the lines to overlap, but that's just cosmetics). The trajectory of the entire West being the same as Italy's is immediately apparent.
In part, because they think they already understand the situation, and the nature of that understanding precludes taking things like that seriously.
“It’s just the flu”
“It only kills 2% of people”
“The flu, cancer, car accidents, malnutrition, etc have killed far more people”
“People were worried about SARS, Swine Flu, and H1N1, and they turned out to be hardly kill anyone.”
“There number of cases here is small. Why are you panicking over nothing?”
“People need to stop panicking. People are going hysterical. The media is trying to make people panic. Just look at them hoarding toilet paper”.
“People are trying to ruin the economy over nothing”
“The experts — epidemiologists — say there’s nothing to worry about” (I’ve had this said to me and I was given a link to a news article that spun statements from some epidemiologists to make it sound that way. They were saying that they didn’t know how the situation would pan out, and this was presented as if it meant they didn’t think there was any issue).
I imagine that most people aren’t aware of the graphs. I imagine most people would be dismissive of them for reasons like the following:
They simply believe the apparent normalcy in front of them more than some abstract maths. They don’t grasp the notion of exponential growth, so it seems fanciful. They also don’t understand how it’s possible to project into the future like that. Maybe they think it’s just fear-mongering speculation. What concrete evidence do they actually have for the situation in Italy? And why should they believe what’s going on in a different country will apply to their country. Maybe their country has a good health care system, and they assume that Italy doesn't.
I've worked with, presented, and consumed a lot of scientific data over my career and I still have a tendency to assume plots are linear no matter how many times I tell myself to always check scale first.
Any half-decent plot aimed at non-specialists will have "log scale" written in the title or surrounding description. The one linked by 'soVeryTired didn't, which is where FT dropped the ball. But it does not matter here.
The relevant axis on this chart is the time axis, the x axis. The chart is linear in it. You see a bunch of nearly identical trend lines, and you have to just count how many days a given country is behind Italy. It doesn't matter what scale the vertical axis is in.
I didn't mean a non-specialist as in an average Joe; I meant an above-average Joe with some interest in one or more of: economy, physics, electronics, mathematics, biology. There's loads of such people.
It's much worse than that. Italy's health system is already collapsing at 20,000 victims. The population of Italy is 60 million. That has to level off at some point due to saturation, but that's at somewhere in the millions or tens of millions.
FWIW, at the moment it's only lombardy's health system which is collapsing, because most of the victims are concentrated there and the growth rate there was _much_ faster because the lock down was only imposed late.
The growth rate is the same in other regions but delayed, and there is some hope that the rest of the country might be able to cope with it better if the lock down measures are effective.
Hopefully. But the health care system in Lombardia has to be the best or at the top of entire the country. Southern Italy will struggle with fewer cases.
Well Lombardy does (number 2 in the regions of the EU). I believe that some Italian commentators have said that one of the biggest reasons for the total country lockdown was that the health systems of Southern Italy were much much worse than Lombardy, and would definitely not be able to cope.
"Normalcy bias can cause people to drastically underestimate the effects of the disaster. Therefore, people think that they will be safe even though information from the radio, television, or neighbors gives them reasons to believe there is a risk."
People just don't want to believe a disaster is about to happen. They will grasp at straws to explain why everything is going to be fine.
That's usually not a problem because disasters are rare, but it will catch us under-prepped when an actual disaster happens.
I have one issue with or maybe just question about this graph. Why it starts with 100 detected cases? It seems like arbitrary round number, but it also seems to be the smallest arbitrary-looking number that makes SK overlap other countries. Why is that? Why is the initial slow spread in SK irrelevant? What caused it to be initially slower than in other countries?
It's somewhat arbitrary, but you can't start from "patient zero" because that's not usually known. And the detailed circumstances of the first few patients matter. By 100 or so, the disease is in the population and starts to behave statistically. That's what's called "community spread".
People infected with the coronavirus tend to vary wildly in how many other people they infect from people who stay home with a fever and infect nobody to "super spreaders" who many infect hundreds of others. That means the spread rate when you don't have a statistically significant number of cases is going to be all over the map naturally and not really comparable.
It’s somewhat arbitrary, but also, countries can’t detect the presence of coronavirus when just a single resident has it. 100 is a good starting point for “this country has detected the virus within their borders — what’s going to happen?”
This doesn't really matter, you're just doing that to make it easier to compare. Shifting South Korea so it doesn't overlap the other countries is possible but not terribly useful.
They do seem to be missing Denmark though, which should stick out somewhere top-left of Norway.
They do seem to be missing Denmark though, which should stick out somewhere top-left of Norway.
I was just talking, via text, to a friend in Norway. They're going for major restrictions on contact and the people there are not worried enough yet. I sent her that graph.
Norway is going into full lockdown (stay at home, don't hoard). Borders closing except for export/import from Monday. Hut vacations now getting banned as well.
Which is a good plan and similar to what Denmark is doing, ie. stay at home as much as possible, everyone who can work from home does so, closing the borders for all non-essential traffic, and so on. There is a whole system being set up for compensation to concert venues and other businesses who are severely hit by the lockdown and blanket ban on gatherings of more than 100 people.
Open air walks are ok, as long as you keep a reasonable distance to other people. Only go shopping if it's absolutely necessary.
And yet some people are still going to crowded bars, like nothing's going on. It's amazing how stubborn some people are.
The graph can be reproduced with more recent data here [1]. It is based on WHO data, and lags a bit behind. If you want to see more data and graphs, see [2].
As a physicist, you are familiar with formulas similar to this:
N_obs = p_detect * 2^( n_days / T_double )
N_obs : The number of observed cases
p_detect : The fraction of actual cases that are detected (assumed to be constant)
n_days : number of days
T_double : The number of days it takes for the number of real cases to double
If you examine the formula, the p_detect constant is almost insignificant. If T_double = 2, a difference in a detection rate of 0.2 and 0.8 is only 4 days for n_days.
As long as T_double is less than several months (and constant), an absolute catastrophy will occur. Within a weeks from now, nearly the entire fraction of the population that is receptive to infection will get infected, and will be sick basically at the same time. With 10-15% of the population requiring intubation, we can end up with a significant part of the population in each country ending up dead.
I believe you're focusing on the days aspect of that equation without considering what a lower T_double/p_detect could mean relative to hospitalizations.
If the real number of cases is doubling significantly faster than those detected -- say due to not testing them because their symptoms are mild enough to be missed entirely or to not seek treatment -- the calculations around things like mortality rate and severity of illness may yet change. As I understand it, scientists have already identified mutations of the virus that may also impact its ability to spread or injure infected hosts. I should note that these changes can swing both good and bad, I'm simply pointing out that there are more variables and that these variables changing may represent something not obvious from the equation.
I'm not an expert; I have fun reading about medical statistics. Most papers I've read take the time to examine these various confounding factors and what unexpected variations in their proposed equations might mean.
If the number of real cases double every N days, the number of people needing hospitalization is also likely to double every N days. If not, it probably means that the infection rate spread at different rates in high risk vs low risk part of the population, but unless those populations are strongly segregated from each other, that is unlikely.
This could go in both directions. In both cases, though it would require that the high-risk subpopulation is primarily infected by each other (or staff) instead of being infected from the general population. If high-risk individuals are primarily infected by low-risk individuals, the doubling time for each group should be the same.
Note that such an effect could go in both directions. The high risk subpopulation could get it at a higher rate the rest if we let the infection spread like wildfire in hospitals and elderly housing centers, or it could spread at a lower rate if the risk patients are kept isolated.
The point is that the mortality rate estimates are going to be totally out of whack without accurate measurements. As well as estimates of the currently infected.
This matters a lot. The first number is obviously important. The second matters so Italy can plan for whether things have peaked yet, or how many weeks out until it does.
The mortality does matter a lot if we plan to let everyone become exposed. However, if we do that, we must expect 15% of the people that are currently having enough symptoms to be diagnosed in Italy to perish. Even if only 20% of the infected are diagnosed there now, that is up 14 million people in Italy (if everyone gets it), out of which 2-3 million would die.
Or, if applied to the US, 10 million.
Alternatively, we can shut down the virus in the same manners that China, South Korea or Singapore have been doing, and keep it supressed until we develop efficient treatment.
Unfortunately, that means shutting down all affected regions really hard, and maintain a high level of supression for maybe 2 years.
However, if we are going to do so anyway, both the human and economic costs will be lower the earlier we begin.
If we allow exponential growth to continue with a doubling time of only a few days (even if we can move it from 2-3 days to 6 days), the time until this move is forced is very limited.
That assumes you are sampling uniformly, and not in already saturated clusters. The doubling time is also not a known constant, as it depends on actions taken etc, and uncertainty in it will broaden the distribution.
Obviously, all this is basic statistics and should be known to epiodemiologists, who hopefully have some input to policies.
For large N_obs, this will maybe be less important as you're going to find the severe cases anyway, but the uncertainty is significant in the beginning stages, and it is unfortunately these stages where actions will have most impact.
As long as growth remains linear in an exponential plot, you are nowhere near the saturation point. When about half the population is already infected, the number of new cases should grow roughly linearly. In Italy, it seems to still grow exponentially.
Itally has already passed the number of simultanous cases that their healthcare system can handle. I don't believe they really want to find out at what level the saturation point can be found. That could mean hundreds of thousands, potentially millions, dead.
Who is this mr Pueyo? And why should we listen to him regarding this subject?
From his Medium profile page it seems he is a 'Storyteller' and 'Viral marketer'. So, someone who knows how to tell a story with confidence even if you know nothing of the subject.
I'm gonna listen to my government regarding this, rather than medium posts by viral marketeers. Thank you.
Looks like NL has had steady exponential growth over the past week or even 10 days.
As far as Mr Pueyo, in this context he appears to be an effective science writer, which is what matters. If you want a more succinct source from an academic, there's http://ctbergstrom.com/covid19.html .
No one is 'confident' about a lot of things. But everyone who has seen what is happening in Italy is confident that taking a 'wait and see' attitude will cost lives.
Why even test? The decision procedure is the same: treat the ill, lock down everyone else at home, avoiding social contact at the max; enforce social isolation and/or masks in "critical" spaces (power plants, grocery stores, ...). What does a positive or negative test change?
Most complete lockdown would seem to coincide with health care system stress beyond a certain level.
Universal testing and full identification, isolation, and clearance of all patients across multiple checkpoints would result in the fewest number subject to confinement, confined in the least broad of areas for the shortest periods of time.
OTOH if insignificant testing has been achieved, lockdown itself will need to be inversely universal and long-lasting.
There is an exponential component involved, so the effect will be felt sooner than you think.
Theoretically either way, it's possible no one will be able to be unconfined across multiple checkpoints without a real-time valid negative test or credential.
That decision could be the same either way.
But the fewer and less reliable the tests, the fewer the number of citizens that can be expected to be allowed to move about with some freedom.
After pandemic stress exceeds the magnitude where there can be no treatment resources for additional patients anyway, movement will certainly not be relaxed, and those who might have had a chance with earlier & more thorough action & testing will be left to expire undertested in confinement.
Not every scenario is that uplifting.
Due to the excess rate of confinement resulting from inadequate testing, the greater stress on the marginal economic needs of a large contingent of the populace may result in a need for lockdowns to become oppressive enough to theoretically halt the spread of all possible crime in addition to disease.
Depends on how serious it gets, if it's bad enough you could get unrulyness or looting like there is during some disasters regardless.
For the first question, the answer is: ANY country that currently is seeing exponental growth should take action at the same level of severity as China/Korea/Singapora, if not, they will be in the same situation as Italy in 1-3 weeks.
Once the growth is no longer exponential, measures can be rolled back slowly, especially if they have access to enough tests, masks and respirators.
The earlier action is taken, the cheaper it will be to stop this. Every week of delay can increase casualty rates by a factor of 10. A month of delay, can mean the difference between 10000 and 10 million dead.
Also, economic costs, both in direct treatment cost as well as the disruption to the productive side of the economy will rise sharply the longer we wait. (Well, at least if we don't see the death of sick and elderly as an economic benefit.)
People will continue to get the Flu, Colds, HIV / AIDs even throughout this whole shebang. We need to know COVID19 cases specifically, to know if our lockdown methodology is being effective.
Exactly. I don't see how trying to limit testing to people who had contact with known cases or traveled to at risk countries (as practiced in Germany) can be successful.
Are you sure that Germany does not perform extensive testing? I admit that reddit comments should not be used as sources but I would love to know more about German approach to testing.
Earl_of_Northesk:
The RKI is conducting random sample testing to keep track of Influenza in Germany. These tests now also test on COVID-19. So far, not a single prior undetected case of COVID-19 has shown up in these samples. It is thus highly likely that the extensive early tracking and testing means that Germany has, in comparison to other countries, a very low rate of undetected cases, which would obviously lead to a lower mortality rate. That's what the President of the RKI also said in todays press conference together with Angela Merkel.
Painy_:
How big is the RKIs sample size tho?
patientzero_:
All cases that had the flu and went to the hospital. So the more severe once. But they also re-ran the tests from the beginning of the year to test for Covid-19. If you can't detect it in there it wasn't in the country most likely
Sounds like a massive amount of testing that no other country can match.
For some context, researchers in China went back and reran old flu surveillance samples from Wuhan taken in December and the start of January. According to the WHO joint mission's report, 1 out of the 20 samples from the first week of January and 3 out of the 20 samples from the second week tested positive for Covid-19. China locked down Wuhan on the 23rd. Things were probably already really bad by that point in a way that wasn't reflected in the number of confirmed cases.
If the availability of testing kits is low and the ratio of infected to non infected people is extremely low, it makes absolutely no sense to sample randomly from the population.
How many do you need though? If you take 0.1-1% of your testing capacity, those handfuls of samples a day give you some information. Not regional level or very reliable data, but it gives an idea of whether people (as a population) are having it and are having mild symptoms and are not reporting anything, or if it isn't widespread yet and the hospital cases are the only cases.
Aldo if you expect the true positves to be a small percentage (which should still be the case in most countries), false positives will dominate in a ranom sampling. Apparently false positives are high for unsymptomatic cases. Of course if you can estimate the false positive rate well enough, the random sampling might still give useful statistics.
As far as I know lab performed PCR tests are assumed to have 0% false positives and about 29% false negatives.
Antibodies tests have about 10% false-positive rate but to the best of my knowledge countries in Europe widely use PCR tests.
I think most places are switching from testing known contact/at risk countries to testing people in hospital with the symptoms. The first strategy makes sense if you're trying to contain a small number of cases, it doesn't make sense once people are catching it from other people in the area.
If you make a bunch of assumptions about the distribution, you don't need a large sample size to make decent estimations about the population. Of course, the only way that works is with random or stratified random sampling. With reporting bias, I'm not sure any country has enough data to make statistically confident statements with any precision.
Folks with a stronger statistics background are welcome to correct me.
It's interesting that you lead by saying "as a physicist".
As a physicist I'm used to thinking about orders of magnitude and whether something grows like log(N) or N!. I'm pretty sure all the data points to this being O(a big problem) but I'd leave it to the epidemiologists to say anything with confidence.
So, as a physicist, you should know how exponential growth works. Let's say you have a pile of Uranium that's juuuust sub-critical. You would likely to be confident to stand next to it without significant fear.
But if someone throws on just enough additional Uranium for the pile to go supercritical, you would run for your life because none of the following will matter[1] all that much to the final outcome:
1) How much neutron radiation there was to start with.
2) The specific exponential growth coefficient.
3) How much total Uranium there is, as long as it's a nontrivial amount
4) Whether your Geiger counter is off by some constant factor or not.
None of those matter. It's going boom. It might go boom a bit sooner or a bit later, but it is going to go boom. That's just how exponential growth works. There's no maybe. There's no "let us wait and see". There's no "we'll hope for the best". No: It. Will. Go. Boom.
All of the factors that are irrelevant are just shifting a figurative vertical wall on your graph paper a bit to the left, or a bit to the right. It's adding or subtracting "a couple of doubling times". If the doubling time is short, then you're not really achieving anything by fiddling with constant factors.
With the Coronavirus just about every country has a doubling time of 4-5 days.
I live in Australia, where we're about a "month behind" everyone else. So of course, the dumbass government is saying things like "the heat here will slow it down". But it hasn't, our doubling time is 4.75 days at the moment. They're saying that it's "premature to lock down the country". No it isn't, it's already weeks too late and getting literally exponentially worse daily! They're saying that the hospitals are being prepared, but no amount of extra beds or ventilators will help. If they double the number, it just delays the catastrophe by 4.75 days. Not even a whole week! Quadrupling beds and ventilators buys just under 10 days before people are being turned away to go home and die.
So, again. I ask you: If you were the nuclear physicist in charge of a nuclear pile and someone told you it's gone critical and the radiation is rising exponentially, is your first reaction to: just "stand around and wait and see what happens", or to: take drastic action right this second? Do you SCRAM, or do you call the communist party leadership for permission? Are you the hero of the Chernobyl story, or the villain?
[1] Ignoring thermal effects slowing down the reaction. This actually has an analogy with disease spread, where there are fewer susceptible people remaining because everyone is already sick or dead. If we reach this point, we'll be seeing millions infected and hundreds of thousands dead.
I think this insight is exactly why the UK health experts are not advocating extreme measures yet. They know they will only delay the takeoff and they need to use those measures when it does, not beforehand, and these measures are meant to protect the most at risk from dying from the disease (I think the most contentious thing is how long these measures can work for. The UK experts are of the opinion they have a finite life).
Keep in mind, the UK advisors think the peak is maybe two months away, and that at-risk groups may need to self-isolate for a month either side of that peak. This is a far bigger response than any country has achieved so far (and it's extra difficult because the at-risk groups are probably the most dependent on external aid, as well as already lacking social contact). I don't think they're wrong to think that this will be difficult to achieve, and increasing the difficulty by starting earlier will make things worse.
There is no SCRAM button on this pandemic, not any more at least.
"This is a far bigger response than any country has achieved so far (and it's extra difficult because the at-risk groups are probably the most dependent on external aid, as well as already lacking social contact)"
How have they achieved this?
What concrete measures?
They haven't yet (no-one has). The point is they are recognising that such measures are very hard on people, and so they don't think they can stay in force indefinitely.
Well, if I try hard to imagine how they think, without assuming incompetence, it would be as follows:
Assumption 1: Our country will not be able to take measures that are extreme enough to stop exponential growth.
Assumption 2: Once a certain level is reached, we can drastically lower the doubling time so that the number of simultanious cases are kept below what our healthcare system can handle.
Assumption 3: If we stay below the level that the healthcare system can handle, mortality rates will be low, maybe lower than 1%.
Assumption 4: The total number of individuals that will require hospitalization is low enough that the healthcare system can treat all patients needing treatment in a few months.
If assumptions 2 is not met, the mortality rates of pations that require treatment is likely to be similar to what is seen in Italy, ie roughly 15%.
If assumption 3 is wrong, and the real mortality rate is about 3-5%, having about half the population infected, will still lead to huge numbers of dead, more than the population is likely to accept.
If assumption 4 is wrong. Italy is currently unable to handle 20000 cases. A country like the UK may be able to handle maybe 10000-20000 simultaneusly. If 10% of the population requires hospitalization, and each patient will stay there an average of 1 month, measures will have to be dragged out over several years, anyway.
Assumption 5: This only needs to be done once, meaning there will not be second or third waves or mutaded viruses that will need to spread in a similar fashion in the same time period.
At some point, I think every country will realize that they need to take drastic measures, enough to stop the spread from being exponential. Doing that after detecting 100000 cases is VERY different from doing it after detecting 1000.
The downside, of course, of preventing exponential growth, is that most measures will have to be kept in place until there is a vaccine or other cure, and that could take 2 years.
The growth will always be exponential. What you can change is the exponent. I don't think they are crazy for suggesting that extreme measures are unsustainable and their use should be timed correctly. I'm not completely sure they're right, but neither am I sure that extreme measures are right. Keeping a quarantine on a whole country up for 2 years seems unlikely. As I understand it, this plan hasn't just been hastily put together overnight, a team has spent a while researching and modelling outbreaks in preperation for just such a scenario, and as such I am inclined to trust them more than politicians (who are always happy to be seen to be doing something about a problem) and laypeople on the internet.
Growth does NOT have to be exponential (or at least not with any near-constant exponent). Furthermore, if the doubling rate is half a year or more, it really does not matter that much if it exponential, unless the number of already infected is already huge, since a vaccine is likely to come within 2 years.
From my perspective, it appears that politicians do NOT want to take sufficiently drastic measures, as the economic consequences will be huge (let's assume that Spain and Italy will keep or increase the measures they already have for 2 years), and so far, their measures do not seem to be sufficient.
Most people will not go to the hospital, they'll stay at home and they wont die unless they dont drink water and eat food with poor nutritional value.
That's why I dont understand the crisis communication on the subject. I understand exponential growth, I dont under and the panic about getting sick with a flu like virus.
If it was something causing skin lesions I'd be in panic mode because the victims would be at a higher risk of co-infectious diseases. This is not that. But hey, fuck my civil liberties some more, for that matter fuck my freedom and that of my countrymen. I dont give a fuck anymore.
Most people aren't susceptible to dying from this. They are likely to spread it. Those who are susceptible to dying from this number in the millions. You can worry about your civil liberties and freedom after you worry about infecting someone who might die because you decided that the personal risk to you wasn't worth a few weeks of inconvenience.
A lot of people have similar statements, but the use of the word "most" in this context just doesn't matter past some cutoff. The flu is very far on the safe side of that cutoff, and the coronavirus is very far on the bad side.
The flu and the common cold virus behave comparably to the current pandemic. The flu in particular kills about 300K per year after infecting about 20% of the global population. That's a mortality rate of 0.02% and a survival rate of 99.98% for the general population, which is not a fun statistic, but nothing to panic about either.
Critically, the hospitalisation rates for the flu are so low that the current infrastructure can handle it. People still die, but only if they couldn't be saved with medical intervention. Much of the time they will receive treatment and live.
Even if you shift the numbers around a lot -- say, 50% infection rate -- the orders of magnitude come out to about the same. Governments can just put out ad campaigns to encourage people to get the flu vaccine to compensate for a particularly bad flu season.
The critical thing with the cold and the flu is that they move well past the initial exponential growth phase into a "logistic curve" long before the hospital systems become overloaded with the sick. That is, each new strain of the flu runs out of victims by hitting the population ceiling of 7.6 billion. Not everyone is vulnerable, and the rest either become immune or protected by herd immunity.
Now compare this to the Coronavirus. It has a mortality rate of about 0.8% of confirmed cases, with medical care. Much more importantly, about 10% of the confirmed cases required intensive care.
Nobody really knows the ratio of confirmed-to-real cases, but I'll be generous and assume that only 20% of all cases get a confirmed diagnosis, with 80% of cases just shrugging it off as a case of the "sniffles". Similarly, I'll assume that the virus will halt at around 20% of the total population.
For Italy, with a population of 60M people, that's 12 million infected, equivalent to 2.4 million confirmed cases, 240K in intensive care, and 19K dead.
But I lied.
I lied when I said "240K in intensive care". There just aren't that many beds, or intubation kits, or CPAP machines, or even oxygen masks. There aren't anywhere near enough doctors, or nurses, or any resource you care to name. I know this to be true because all of these things have run out already.
Long before the exponential curve starts to "slow down" and become logistic, the entire medical infrastructure becomes overwhelmed and the cases that "would survive with intensive care" turn into "deaths".
Worse, this happened at a "confirmed case count" of about 10K. I said 2.4M above!
The conclusion is that the Coronavirus can overwhelm medical systems waaaaaaay before it hits the "knee of the logistic curve", making it a nearly pure exponential curve. Exacerbating this is the incubation time, meaning that any measure taken today will have essentially no effect for at least a week.
Act now and save lives, act tomorrow and see your loved ones die.
There are more cases, they are on average much more mild, the real mortality rate is much lower, it is actually not doubling every two days (it is the tests that are doubling every few days). Lots of possible and very consequential conclusions.
But with several weeks worth of lag. The number of deaths today should be divided by the number of cases N>10 days ago. The number of cases was much more severely underestimated N days ago than today. The death rate in Italy is basically unknown because the denominator is just noise with a time lag.
As someone who's dealing with analytics data regularely, thank you !
i absolutely don't understand how can someone give any ratio about this disease knowing how only the most severe cases got tested ( except in SK), and that the symptoms are almost undistinguisable from the flu.
i wonder if it's really true that "few people" have it. We do observe a huge amount of people going to the hospital in italy, but that could very well be because we reached the peak of the epidemie, where almost all of the population have been infected and remain asymptomatic.
in this hypothesis, you implement a lockdown and see number drops over two week but what you're really seing is a population reaching herd immunity.
When we are getting close to the peak of the epidemic, the growth will no longer be exponential, but close to linear. A logistic curve looks exponential for about the first 3rd, close to linear for the second third, and then approaching the asymptote with a negative exponential growth for the last third.
Increasing social distancing will naturally lower the exponential growth rate, but unless the growth becomes linear, there is no reason to believe that herd immunity is anywhere close.
In the asian countries, we more or less know that they have been able to contain the virus, instead of waiting for herd immunity. That meanst that they must have found most of the infected cases (or at least quaranteened them). This gives a good indication of how many deaths are caused by a given number of infected. The numbers are not different enough from Italy to think that more than (at most) a couple of hundred thousand in Italy have reached immunity. If so, it means that we have about 2 more orders of magnitude of growth before herd immunity can be reached. That would be hundreds of thousands of dead, if not millions, just in Italy.
That would be for a homogeneous spread inside a country.
However if the epidemic spreads from region to region, you could reach a local herd immunity in the first regions infected way before seing the country-wide curve becoming linear.
But thanks, trying to find a counter-argument to your post made me realize a single-curve model probably doesn't make a lot of sense to try and understand accurately the spread of an epidemic.
There aren’t large numbers of random people testing positive for it where they’ve done wide spread testing. Korea in particular probably has close to an accurate count, and their mortality rate is still close to 1%
What do you think of the practice of only testing people who need hospital-level care and people who had contact with confirmed covid-19 patients (and people who traveled to at risk regions)?
I would think that this can only give you the infected from a few clusters and you can be surprised by an unknown cluster of patients suddenly needing intensive care.
Edit: And due to the long incubation period, that cluster can be quite large.
Testing the entire population is not viable. If you don't have many in-country cases, you can delay the epidemics arrival by controlling just the people that come from elsewhere.
Of course, after the disease starts propagating internally, testing becomes irrelevant, and it's time to reduce its spreading speed.
{kind=link}
It seems only SK has earned that right and has tested enough people to get reliable statistics. If you only measure the sick in the hospital...